“The Radiochemistry of Uranium” by James E. Gindler
Old school technical reference book on uranium chemistry.
Source ☢️: moltensalt.org/references/sta…

If you don’t pursue safety in a way that is cost effective, you are killing people. -- [David Okrent, Past chairman, Advisory Committee on Reactor Safeguards]
Suppose early in 1979, you asked yourself what is the most definitive experiment we could do to learn about the radioactive harm associated with a nuclear power plant release. The obvious answer: a big release would be that experiment. But you would immediately reject that idea on both ethical and economic grounds. Since then we’ve inadvertently run that experiment three times. Let’s look at the results. //
Three Mile Island, Chernobyl, Fukushima //
So we did the definitive experiment. The result: even in a very large power plant release, dose rates to the public are almost never higher than the dose rates our bodies know how to handle. Nature had to equip us with those repair systems to cope with the onslaught of DNA damage from our internal metabolic processes, which damage our DNA at a rate that is at least 25,000 times higher than the damage rate from average background radiation.
Nuclear power plant casualties are extremely expensive economically, which means it’s in the operators’ interest to build robust plants and operate them prudently. But from a public, radiation point of view almost all releases will produce no detectable harm, and the very worst releases are no worse than a bad refinery fire at killing the public.
This puts nuclear in the same category as wind and solar, when it comes to directly killing people per TWh of electricity, and orders of magnitude less directly deadly than coal plants. But it’s the indirect deaths that really count. The easiest way to kill a lot of people is to make them poorer. With a few exceptions, wind and solar will do that. Nuclear will too unless it is as cheap as coal. Nuclear has been cheaper than coal, and can be cheaper again; but only if we regulate nuclear in a way that eliminates barriers to entry and forces the vendors to compete on an even playing field. Right now we are doing exactly the opposite. We are killing people.
The Rockefeller Foundation and its allies decided to argue that radiation produced genetic damage and that damage was unrepairable. Radiation damage just keeps building up. Therefore, the harm was proportional to the total dose, regardless of how rapidly or slowly that dose was incurred. This is like saying taking 365 tablets of aspirin at once is the same as taking 1 tablet per day for 365 days. This no repair hypothesis is called the Linear No Threshold model or LNT.
If LNT is correct, then the Banners could aggregate the tiny increases in dose rate due to test fallout over hemispherical populations and over decades to argue that Bomb testing was invisibly killing millions of people worldwide. The Foundation expertly (and unscrupulously) promoted LNT with all its resources.
adiation. Should I be concerned about it? Is it safe? Is it harmful? How do I know when it is okay and when it isn’t? Some people say it is nothing to be concerned about, but others say even a little is too much—what should I believe?
We all have questions about radiation and it isn’t easy to sort through the available material to find answers. Sometimes the information is too technical or it is too hard to find just the answer you’re looking for. The purpose of the information on this Web site is to help you find answers quickly and easily.
The radiation warning symbol should not be confused with the civil defense symbol designed to identify fallout shelters. For more information about the latter, view the collection item Civil Defense Fallout Shelter Sign.
Radiation Warning Symbol (Trefoil)
Radiation warning symbol
The civil defense symbol for a fallout shelter consists of a circle divided into six sections, three black and three yellow. The general form is very similar to the above however there is no central circle. The Office of Civil Defense originally intended fallout shelters to use the radiation warning symbol with the circle in the center and the three blades, but this idea was rejected because a fallout shelter represents safety whereas the radiation warning symbol represents a hazard.
The three-bladed radiation warning symbol, as we currently know it, was "doodled" out at the University of California Radiation Laboratory in Berkeley sometime in 1946 by a small group of people. This event was described in a letter written in 1952 by Nels Garden, head of the Health Chemistry Group at the Radiation Laboratory: "A number of people in the group took an interest in suggesting different motifs, and the one arousing the most interest was a design which was supposed to represent activity radiating from an atom."
The first signs printed at Berkeley had a magenta (Martin Senour Roman Violet No. 2225) symbol on a blue background. In an earlier letter written in 1948, Garden explained why this particular shade of magenta color was selected: "it was distinctive and did not conflict with any color code that we were familiar with. Another factor in its favor was its cost... The high cost will deter others from using this color promiscuously." Explaining the blue background, he said, "The use of a blue background was selected because there is very little blue color used in most of the areas where radioactive work would be carried out." //
Despite Garden's view to the contrary, most workers felt that a blue background was a poor choice. Blue was not supposed to be used on warning signs, and it faded, especially outdoors. The use of yellow was standardized at Oak Ridge National Lab in early 1948. At that time, Bill Ray and George Warlick, both working for K.Z. Morgan, were given the task of coming up with a more suitable warning sign, a blue background being too unacceptable. Ray traveled to Berkeley and picked up a set of their signs. Back in Oak Ridge, Ray and Warlick had their graphics people cut out the magenta symbols and staple them on cards of different colors. Outdoors, and at a distance of 20 feet, a committee selected the magenta on yellow as the best combination.
The Office of Civil Defense originally intended fallout shelters to use the radiation warning symbol (yellow background with a magenta circle in the center of three magenta blades) but this idea was rejected because a fallout shelter represents safety whereas the radiation warning symbol represents a hazard. The above version of the national fallout shelter sign was introduced to the public by the Defense Department on December 1, 1961. It was intended to only be used with federally approved shelters. Unlike this example, these signs often had yellow arrows below the words "fallout shelter" to indicate the direction to the shelter. In 1962, contracts were negotiated for the production of 400,000 aluminum outdoor signs and one million steel signs for indoors.
The document concentrates accurate information about radiation into a a tri-fold that can be read and understood in just a few minutes. It is a valuable presentation handout, would be a useful addition to the material offered in doctor’s offices, and should be a part of any classroom discussion about radiation.
Robert Hargraves, who has lived a life of achievement including writing a well received book titled Thorium: Energy Cheaper than Coal, founding a business, serving as Chief Information Officer for Boston Scientific, serving as an assistant professor and associate director of the computation center at Dartmouth College, publishing numerous peer-reviewed articles on a variety of topics and earning a PhD in Physics from Brown University, researched and produced “Radiation: The Facts” as a “labor of love”.
Hargraves tapped a deep pool of expertise by requesting reviews and comments from his extensive contact list that includes radiation biologists, health physics professionals, and nuclear engineers. Though space on a brochure is obviously limited, Robert has provided the references supporting the statements on the brochure on his web site and given creative commons license for others to republish his work.
We are writing to express our concerns with a January 30, 2014 article by Rita F. Redberg and Rebecca Smith-Bindman. The article is alarmingly titled, “We Are Giving Ourselves Cancer”, and is accompanied by a frightening cartoon that appears to be a doctor holding an X-ray film, and wearing a gas mask and helmet. The picture and title are the first clues that sensational claims follow, and the article does not disappoint in that regard, though it falls far short in offering prudent medical advice to frightened patients and parents.
The authors only mention in passing that medical imaging can save lives, and quickly move on to assert that there is little evidence of better health outcomes from current scanning practices. They do not mention, for example that the National Lung Screening Trial recently found that former smokers who received CT screening were 20% less likely to die from lung cancer and 7% less likely to die from any cause, compared to those who were screened with lower dose chest radiography. They do not mention the studies demonstrating the clear clinical benefits of mammography, bone mineral densitometry, and CT colonography. They do not mention the hundreds of studies that suggest that the body’s natural defense systems are quite capable of dealing with very low doses of radiation – like those that have existed on our planet since its beginning and those associated with modern medical imaging.

When a single RIF (Radiation Induced Foci) is faced with multiple DSB's (Double Strand Break in DNA), it can end up rejoining the wrong ends, creating a possibly viable misrepair. A few of the viable mutations will escape our immune system, and a few of those could become cancerous.
If double DSB's are the real problem, then dose rate and repair time becomes all important. The probability that a hit will cause a DDSB is proportional to the inventory of still unrepaired DSB's at the time of the hit.3 To over-simplify, if the repair processes can keep up with the damage, and keep that inventory low, we are OK. If the damage rate is higher than the repair rate, the inventory of unrepaired DSB's will build up, and the probability of a DDSB and a misrepair will grow rapidly. //
If we conservatively assume 10 metabolic DSB's per cell-day, and 0.04 DSB's per millisievert then it would take 250 mSv per day to equal the number of DSB's produced by our metabolism. 250 mSv is about 25,000 times normal background radiation. If normal metabolic damage is equivalent to 250 mSv/d, then any damage associated with 2 mSv/d would almost certainly not be detectable. At the same time, it is not surprising that we start to detect harm at 20 or so mSv/d. At that point, the cell is forced to deal with a substantially higher than normal number of DSB's. ///
Nature has equipped us with a remarkably effective DNA repair system. She had to do this because our O2 based metabolism damages our DNA at a rate that is more than 25,000 times the damage rate from average background radiation.
If a radon test detects levels above the EPA’s action threshold (4 pCi/L), a radon mitigation system is typically installed. The most common design is a sub-slab depressurization system. This method uses a combination of PVC vent piping and a radon fan to draw the gas from beneath the building’s foundation and discharge it safely above the roofline, away from windows or air intakes.
The principle is simple but effective: by creating negative pressure beneath the slab, radon is prevented from entering the living space. These fans are often located in basements, attics, or outdoors to minimize noise and provide continuous operation.
However, because the fan and piping are usually hidden from view, it can be difficult for homeowners or facility managers to know whether the system is operating properly. ///
Radiation exposure is non-cumulative beyond a 24 hour dose rate. "Radon mitigation" is just another grift, sanctioned by the government.
Rhetorical question: If radiation is so dangerous (i.e., causes cancer so readily), why do we use it cure cancer? Doesn't it cause more cancer?
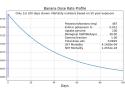
according to LNT, if every human ate a banana a week, bananas would kill 1600 people a year. In the same scenario, SNT kills one person every 2.5 million years.
Now, class, let's get back to basics.
Repeat after me:
It's not dose. It's dose rate profile.
Good.
Repeat after me:
LNT does not say eating a banana is safe or unsafe.
LNT says eating a banana has a 4 in a billion chance of killing you.
Repeat after me:
SNT does not say eating a banana is safe or unsafe.
SNT says eating a banana has a 1 in a billion-billion chance of killing you.
Whether those risks are safe or unsafe is up to you.
Class dismissed.

A 2025-07-12 WSJ article called the Linear No Threshold (LNT) radiation the model, the model that assumes "there is no safe level of exposure to radiation". LNT makes no such claim. LNT converts a dose rate profile into a cancer incidence prediction. That's it. LNT like many other possible models predicts a positive cancer incidence for any dose rate profile whose cumulative dose is positive. //
A far better definition of LNT is: the model that assumes radiation damage to our DNA is unrepairable. Harm just keeps building up. Therefore, the only thing that counts is total dose. How quickly or slowly that dose is incurred is irrelevant.
The no repair assumption was proposed about 100 years ago, at a time when we knew nothing about DNA. We did not even know it existed. We now know a providential Nature has equipped us with a remarkably effective DNA repair system. She had to do this to protect our DNA from our own oxygen based metabolism which produces double strand breaks of the DNA helix at least 25,000 times more rapidly than average background radiation. This repair system can be overwhelmed if the dose rate is high enough; but such dose rates will almost never be encountered by the public in a nuclear power plant release.
LNT denies well established, indisputable biology. In 2018 [2015], Nobel prizes were awarded to three scientists that have been in the forefront of figuring out just how the repair processes work.

If LNT is biological nonsense, how did it ever get accepted? The Hamlet in that tragedy is Ed Lewis.
The Rockefeller Foundation and the Genetic Scare. //
Hundreds of scientists could have pointed out the glaring inconsistency. But as far as I know none did. Moreover, fractionation, dividing a therapeutic dose into fractions, delivered a day or so apart to allow healthy cells to recover, was universal medical practice. If LNT is valid, fractionation makes no sense. Even Lauriston Taylor, a towering figure, who called LNT "a deeply immoral use of our scientific heritage" did not speak out until 1980. He was about 25 years too late. Were all these people grasping creeps?
Of course not. They were petrified of the bomb. If LNT could end bomb testing, then I will have to abandon scientific integrity, just this once. Look at Taylor's strange wording. You don't normally call a model, a "use". He knew LNT had been accepted not because it was correct, but because it was a tool, a tool for controlling the bomb.

Most people do not realize how delayed portions of the Fukushima evacuation were. I certainly did not. By the end of March, the situation at the plant was under control. Power had been restored to the site. The team was getting water to all the stricken reactors. The temperatures were coming down. The release rate was one ten thousandth of what it had been earlier.\cite{tepco-2012a}[p 51]
The government fully expected to restart Japan's reactors quickly. The job was mainly clean up and rebuild from the tsunami. They were quite taken back when the public led by a normally tame press turned against nuclear power, threatening the ruling Democratic party.
The politicians responded. On April 22, 40 days after the start of the release, the government implemented two new evacuation zones, Figure 1. The area out to 20 kilometers from the plant had already been evacuated. //
Figure 2 shows the GKG dose rate profile for the high end Iitate population. GKG estimates the peak high end ambient dose rate for this town was 47 microGy/h, not that much lower than UCS's number for Okuma. According to LNT, making these people evacuate after 50 days increased their life expectancy by 24 days. For most of the citizens of Iitate, the numbers would be lower to much lower. According to SNT, forcing these to people to evacuate after 50 days, increased their life expectancy by 1.7 minutes. The stress of evacuation will be far, far more costly. //
Under LNT, the harm just keeps building up. In a nuclear power plant release, after the initial rapid decline, the dose rate falls off very slowly. The cumulative dose for the Iitate high end group after a 40 year exposure period is 613 mSv. For an LNTer, this is a scary number, since it only took a 150 mSv or so acute dose to produce significant increases in cancer in the bomb survivors. For an LNTer, the fact that the bomb survivors suffered most of their dose in seconds, while the Iitate citizens will receive their dose fairly evenly over 40 years is irrelevant. Given our rate dependent ability to repair radiation damage, this is biological nonsense. //
This is so stupidly tragic that I don't know where to begin. The peak dose rate in the EPA was around 0.06 mSv/d and lasted roughly 10 days. In the Karunagappally study, Figure 4, the people who got 0.06 mSv/d showed no increase in cancer and they averaged that dose rate for at least 19 years. By day 50, when most of these people were frightened into leaving, the dose rate was down to around 0.02 mSv/d. In the Karunagappally study, we have nearly a million person-years at this dose rate or higher with no increase in cancer. And most of these people experienced these dose rates their whole life. //
The people in the EPA had their lives uprooted, and in many cases ruined for no reason at all. Or rather by a model that is tragically misleading. Given its consequences, I have no problem calling LNT evil. What does that say about its promoters?
What I don’t believe is that society needs to seek to reduce either “man-made” CO2 or “man-made” radiation doses to near zero. There are reasons to limit both CO2 and radiation doses, but there is no logical or moral reason to impose too tight a limit on either one.
In fact, I’ve often found that people working very hard to impose such limits don’t even like other people and seek to restrict their access to economic prosperity and physical power.

Human Health and Welfare Effects from Increased Greenhouse Gases and Warming
-- John Dunn and David Legates
Claims that global warming will have net negative effects on human health are not supported by scientific evidence. Moderate warming and increased atmospheric concentrations of carbon-dioxide levels could provide net benefits for human welfare, agriculture, and the biosphere by reducing cold-related deaths, increasing the amount of arable land, extending the length of growing seasons, and invigorating plant life. The harmful effects of restricting access to fossil fuel energy and subsequently causing energy costs to increase would likely outweigh any potential benefits from slightly delaying any rise in temperatures. Climate change is likely to have less impact on health and welfare than polices that would deprive the poor living in emerging economies of the benefits of abundant and inexpensive energy. //
As this chart shows, by a wide margin, the Gasparrini et al. study illustrates that cold extremes kill far more people that heatwaves—and by a wide margin. They concluded:
Our findings show that temperature is responsible for advancing a substantial fraction of deaths…7.71% of the mortality…. Most of the mortality burden was caused by days colder than the optimum temperature (7.29%) compared with days warmer than the optimum temperature (0.42%). So cold produced 17 times the number of heat deaths.7 //
Underlying the concept of Net Zero is the LNT [Linear No Threshold - nuclear radiation] philosophy laid down more than three decades earlier: no net emissions of greenhouse gases are acceptable. There is no threshold that allows some net production of greenhouse gases such that at any level, the net emission of greenhouse gases at any non-zero level is detrimental to the environment and must, therefore, be stopped. The belief is that since urgent action must be taken to avoid any additional warming of the planet, greenhouse gases must be removed from the atmosphere.71 When “emissions released by human action are taking a catastrophic toll on our planet and propelling us further into an irreversible climate crisis,” no threshold is acceptable.72 //
Linear No-Threshold theory began in 1927 when H. J. Muller examined phenotypical damages in fruit flies resulting from x-ray exposure, for which he was awarded the Nobel Prize in 1946.78
Ibid.
It was introduced in radiological risk studies in 1959 and subsequently into general cancer risk. Consequently, the U.S. National Academy of Science recommended use of the LNT model to the induction of radiation-related mutations in somatic cells and, subsequently, to the study of cancer initiation.79
Edward J. Calabrese, “Cancer Risk Assessment, Its Wretched History and What It Means for Public Health,” Journal of Occupational and Environmental Hygiene, Vol. 21 (2024).
In low-energy radiation, The United Nations Scientific Committee on the Effects of Atomic Radiation based its radiological protection system on the assumption that the radiation-induced risk was directly proportional (i.e., linear) to the dosage, with no dose threshold below which no risk exists.80
Dominique Laurier et al., “The Scientific Basis for the Use of the Linear No-Threshold (LNT) Model at Low Doses and Dose Rates in Radiological Protection,” Journal of Radiological Protection, Vol. 43 (2023), 024003.
About a decade after receiving the Nobel Prize, Muller admitted that he did not discover small mutations in fruit flies with the x-ray exposure for which he was heralded; rather, the high-energy radiation nearly obliterated large portions of their chromosomes. However, his Nobel Lecture argued that no safe radiation dose existed and that the LNT model must replace a threshold-dose-response model.81
Ibid., and Edward J. Calabrese, “Flaws in the LN Single-Hit Model for Cancer Risk: An Historical Assessment,” Environmental Research, Vol. 158 (2017), pp. 773–788; Edward J. Calabrese, “From Muller to Mechanism: How LNT Became the Default Model for Cancer Risk Assessment,” Environmental Pollution, Vol. 241 (2018), pp. 289–302; and Edward J. Calabrese, “Ethical Failures: The Problematic History of Cancer Risk Assessment,” Environmental Research, Vol. 193 (2020), 110582.
A Better Rule. An obviously better rule than LNT (and to net zero and other greenhouse gas–reduction strategies) is that of Paracelsus, a Swiss physician and alchemist of the 16th century: “All things are poison and nothing is without poison; the dosage alone makes it so a thing is not a poison” (Sola dosis facit venenum).82 //
Eighty percent of modern energy is produced by burning petroleum, natural gas, or coal to turn the turbines inside electricity generators. (See Chart 2.) Running 24 hours a day and seven days a week, a traditional coal, natural gas, or nuclear plant requires about 12.5 acres per megawatt of electricity. By contrast, solar (43.5 acres per megawatt) and wind (70.6 acres per megawatt) arrays occupy vastly more land area and have a much larger negative impact on the local habitat and its environment.93



Nuclear medicine is one of those cool specialities that doesn’t get enough attention. While nuclear energy has enjoyed a revival in recent years, little attention has been paid to nuclear medicine. That’s probably partly because explaining it in technical terms inevitably removes some of the magic and partly because many people fear radiation and don’t want to think about it.
But nuclear medicine deserves attention. Not all of the world's nuclear reactors are used for producing energy; they are also used for producing radioisotopes for medicine and industry, training, and other purposes. They are known as research reactors, and there are currently around 220 research reactors in 53 countries. In the heyday of nuclear development, in 1975, there were 373 neutron factories in 55 countries. //
Outside of the wealthier nations, there is a significant shortage of equipment and workforce for nuclear imaging around the world, and one study found that:
A comprehensive scale-up of imaging, treatment, and care quality would avert 9·55 million (12·5%) of all cancer deaths caused by the modelled cancers worldwide, saving 232·30 million life-years. Scale-up of imaging would cost US$6·84 billion in 2020–30 but yield lifetime productivity gains of $1·23 trillion worldwide, a net return of $179·19 per $1 invested.
Healthy people benefit humanity. For those living in the poorest nations to gain access to improved healthcare, nuclear medicine will play a vital role going forward, although when and how that will happen remains to be seen.

In reporting on a radiation study, a nearly universal practice of the 'experts' is to show us only the subjects' total doses. They do this despite the fact that usually what is measured is the dose rate profile, often in the form of daily doses. The total dose is computed by adding up these daily doses, and then tossing aside everything but the total. Analyzing radiation harm by only looking at total dose is like an electrical engineer attempt to analyze a complicated circuit by only looking at the annual energy input.
The human body is an extremely complex circuit. It has to be analyzed dynamically. The essential element of SNT [Signmoid No Threshold] is not the shape of the acute dose response curve, it is chopping the dose rate profile into repair periods, and analyzing each period separately. //
Where would we encounter 1 and 2 mSv/d dose rate profiles for decades? That's an easy one. Space travel. The astronauts in Low Earth Orbit get between 0.5 and 1.0 mSv/d, with occasional spikes during solar flares. High Earth Orbit or a trip to Mars will about double that. If LNT were valid, the shielding requirements would be prohibitively expensive.
NASA can't afford LNT. That's why it ignores all the EPA and NRC limits. The EPA says more than 1 mSv per year is unsafe. NASA says 1 mSv per day is routine. That's the difference between the top and bottom of Figure 1.
NASA is not the only entity that cannot afford LNT. Space travel is a luxury that humanity may or may not be able to afford. The benefits of manned space travel are at best speculative. The benefits of cheap nuclear electricity are undeniable and cornucopic. If we can correctly trash LNT to go into space, surely we can junk this counterfactual hypothesis to get cheap nuclear.
What is Radiation Dose?
When people talk about dose, they're usually using sieverts (or rem, if in the US). Sieverts (Sv) are best used for external doses, like say the dose you receive from a giant hunk of radioactive cobalt across the room.
To understand sieverts, you should first understand grays (US equivalent: rad). 1 gray is equal to 1 Joule of energy per kilogram of matter. Energy/matter provides an idea of how much effect the radiation has, scaled for the size of whatever it's hitting. Sieverts include a quality factor in order to take into account the biological effect of the radiation (1 Sv = 1 Gy*quality factor). Alpha particles have a quality factor of 20, because they deposit all their energy in a small area. Gamma rays and beta particles have a quality factor of 1, because their energy is more spread out, meaning the tissues struck by gamma rays are more likely to recover. So, while different types of radiation have different effects, 1 Sv of alphas is equivalent to 1 Sv of gammas.
Contamination is a little different from radiation. Radiation consists of tiny invisible particles, the largest of which is the size of a helium nucleus. Contamination consists of actual atoms or molecules, and is best understood as "radioactive stuff wherever we don't want it". It is usually expressed in terms of counts per minute (cpm) or decays per minute (dpm), and can be separated into "removable" and "fixed", which are exactly what they sound like. Counts per minute are what you see on your geiger counter. Dpm is just cpm corrected for the efficiency of the detector (about 10% on your average geiger counter, should be calculated when the meter is calibrated). At the Reed Reactor, we consider something "contaminated" and in need of cleaning when it's reading 1000 dpm per 100 square centimeters.
The US Environmental Protection Agency (USEPA) is the primary federal agency responsible for promulgating regulations and policies to protect people and the environment from ionizing radiation. Currently, the USEPA uses the linear no-threshold (LNT) model to estimate cancer risks and determine cleanup levels in radiologically contaminated environments. The LNT model implies that there is no safe dose of ionizing radiation; however, adverse effects from low dose, low-dose rate (LDDR) exposures are not detectable. This article (1) provides the scientific basis for discontinuing use of the LNT model in LDDR radiation environments, (2) shows that there is no scientific consensus for using the LNT model, (3) identifies USEPA reliance on outdated scientific information, and (4) identifies regulatory reliance on incomplete evaluations of recent data contradicting the LNT. It is the time to reconsider the use of the LNT model in LDDR radiation environments.